Information Availability 2018 Benchmarking Study
Raw Data Results for Questions 1 – 7
Responses to date: 151
Study Objective:
In order to address the changing landscape of Emergency Medicine’s role in the future of healthcare, as well as government regulations, Emergency Departments need timely access to actionable information they trust more than ever. In short, data needs to inform decision making and enable the necessary organizational collaboration to improve performance across a broad spectrum of areas including quality of patient care, service delivery, risk mitigation, and profitability.
A lack of relevant and accurate information can have a direct impact on operational efficiency, the cost per intervention, clinical workflow and ultimately, patient satisfaction. This study was designed to compare the availability of information in Emergency Departments across the U.S. and reveal the potential impact data availability has on Operations, Clinical Outcomes, Finance and Patient Satisfaction. The responses to the survey are intended to uncover where the need for advanced performance analytics lies.
Survey url: http://d2i.c3techtargeting.com
During a recent EDPMA event, Dr. Randy Pilgrim, Enterprise Chief Medical Officer for Schumacher Clinical Partners noted, “Due to an increasingly complex and competitive healthcare environment, it is more important than ever to clearly articulate and quantify the value of what we do. Having robust data sets to demonstrate our value is now a business imperative. This will be even more important as Emergency Departments face increasing competitive pressure and cost scrutiny thanks to the high demand for ‘unscheduled care’.“
Findings in a study from the University of Maryland School of Medicine found that 48% of all healthcare occurs within the Emergency Department. The report highlights that the Emergency Department is increasingly being used for non-emergency cases, with some experts stating that deficiencies in both inpatient and outpatient resources and a lack of effective prevention are the main reason why many seek these services. About 17% of ED cases are not actual emergencies; in some cases, insurance companies will try and prevent people from going into the ED, creating challenges for the landscape.
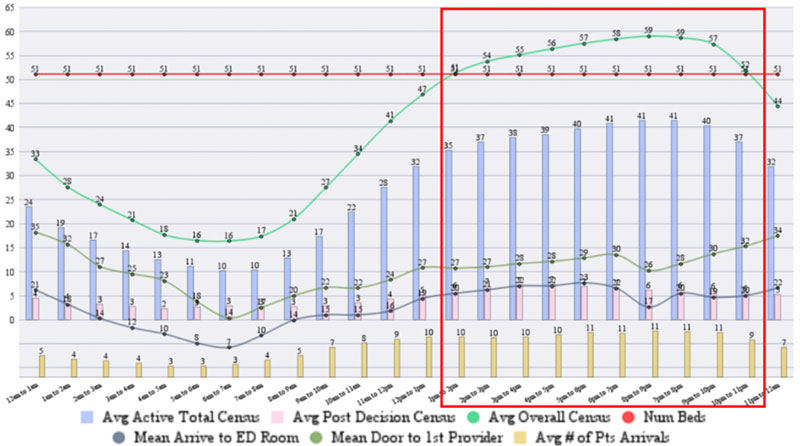
In our own research, the ability to properly assess and analyze these challenges aids in reducing overcrowding within the Emergency Department. The graph to the right shows the average census of the ED by the hour of the day with the green line showing where the census exceeds the number of available beds and boarding is likely to occur.
Summary of Data Results Study:
- 151 companies participated in this study
- Patient satisfaction is a very important driver for healthcare administrators
- 96% of respondents have a Process Improvement Program in place, however analytics for tracking this work is manual, losing valuable time and insights
- Staffing optimization was the highest ranked challenge by ED physician leadership
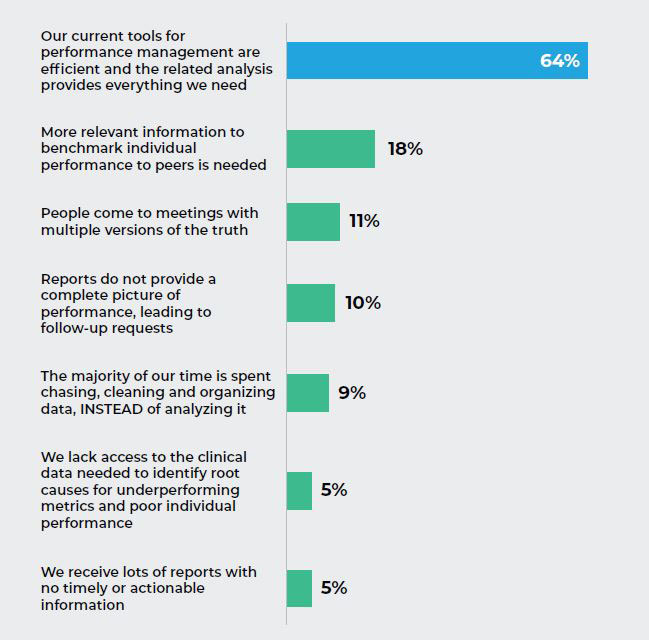
Q1. Which, if any of the following statements describes your Emergency Department’s performance reporting process?
The Insight:
The majority of the respondents who participated in the study believe their current performance management tools are adequate, although many cited a need for more relevant benchmark information. What we learned through more in-depth conversations with many of the survey participants was that the state of maturity in the use of data and analytics was largely limited to static reports and data dumps into spreadsheets.
Nearly 2 hours is devoted to maintaining or managing EHR and other clerical work during the clinical work day, according to a 2016 study from the Annals of Internal Medicine. More than 49% of physician time was spent on EHR and desk work, versus the 27% on face time with patients. The same resource cites, regulatory requirements on EHRs have contributed to dissatisfaction with EHRs.
This begged the question, why were nearly two thirds of the respondents largely satisfied with their current performance management reports? We learned through these conversations and through other survey questions that many of the respondents were unaware that more robust analytics are possible.
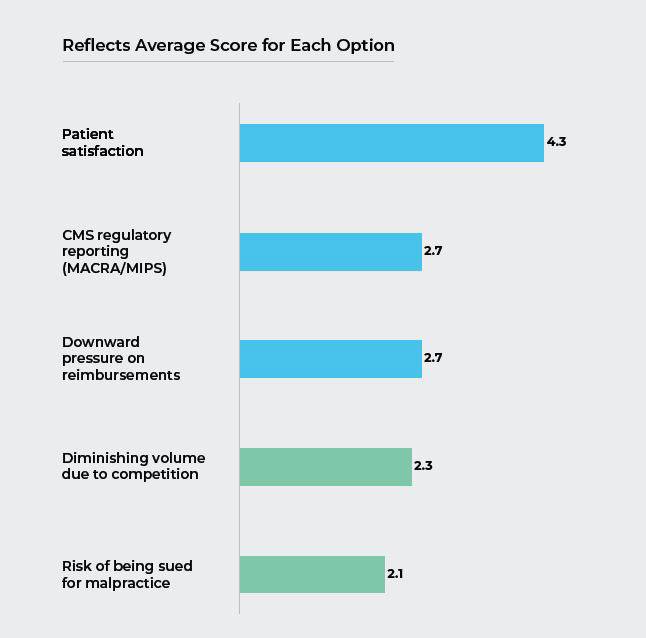
Q2. On a scale of 1 to 5, with 5 being the highest, rate the importance of the following concerns of hospital administration for the Emergency Department.
The Insight:
Not surprisingly with the increased emphasis on value-based purchasing, patient satisfaction was by far the most often cited concern that Emergency Departments needed to address with Hospital Administration.
We believe this also is a function of increasing competition from urgent care centers. Since the ED is the front door to profitable inpatient and ancillary services and CMS Hospital Compare Star Ratings are easily accessible, Hospital Administrations are increasingly interested in protecting their reputation.
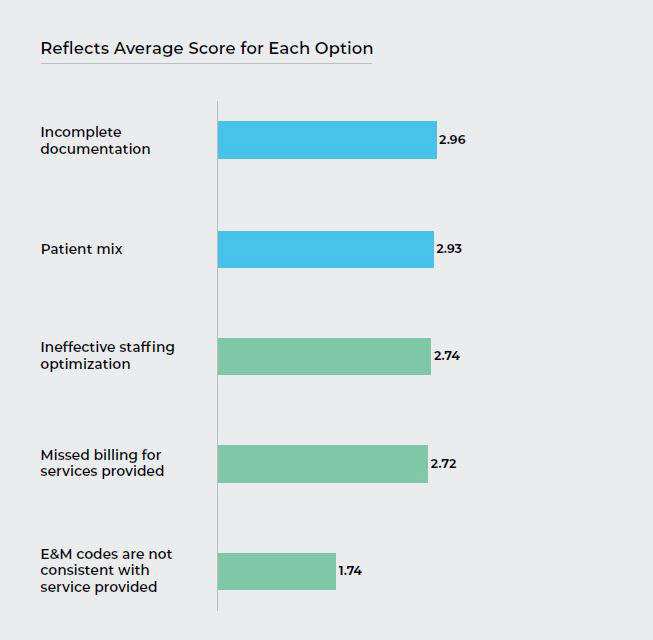
Q3. On a scale of 1 to 5, with 5 being the highest, rate the impact the following challenges have on your Emergency Department’s profitability.
The Insight:
The survey results regarding profitability challenges were decidedly mixed. Although a moderate proportion of respondents cited patient mix as being a drag on profitability some pointed out in the in-depth surveys that this was largely uncontrollable, “You can’t pick your patients”.
Scheduling optimization is gaining interest as an effective means to more effectively put the right staffing mix in the right place, at the right time, creating opportunities to reduce staffing costs and increase capacity at the same time. Most respondents we talked to were interested in staffing optimization but did not have access to the data and tools it requires.
Missed billing for services provided, incomplete documentation and E&M codes are not consistent with services provided all contributed to breakdowns in the revenue cycle. Most respondents, as learned from the in-depth interviews, had no way to integrate claims and EHR data. Without an easy way to augment claims data with EHR data the billing process of manually reviewing charts is not only less efficient but subject to greater human error which can lead to revenue leakage, denials and reimbursement delays.
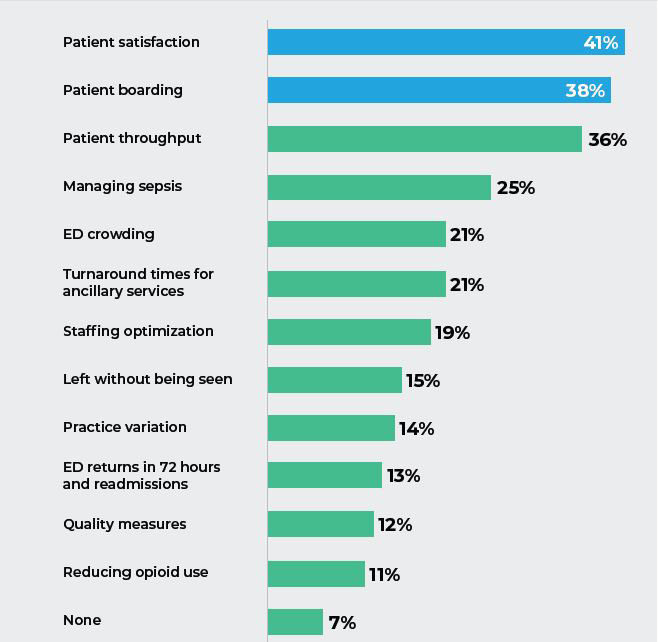
Q4. Which, if any, of the following metrics need Performance improvement in your ED?
The Insight:
In this question respondents had the opportunity to pick multiple items they felt needed performance improvement in their ED. Most respondents picked more than one and some picked as many as 5 responses. Not surprisingly, patient satisfaction topped the list for the same reasons cited earlier. Other frequent responses were related to ED operations; patient throughput, crowding, LWBS (Left Without Being Seen) and less directly turnaround time for ancillary services.
As indicated in the in-depth surveys we conducted, the majority of EDs lack control over ancillary service turnaround times that affect an ED’s patient LOS and contribute to boarding. Further, the majority of respondents felt improving ED operations was either out of their control or they lacked the necessary information to identify specific actions to improve or to have more convincing conversations with other departments.
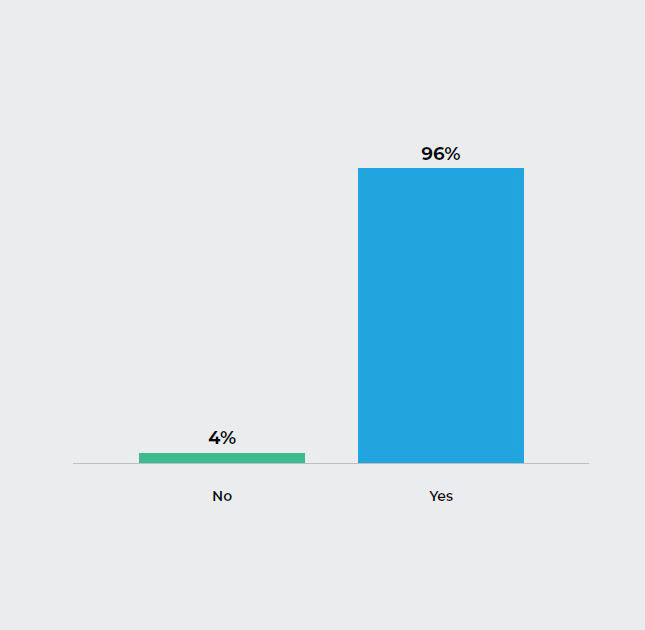
Q5. Do you have a formal Process Improvement program in place in your ED?
The Insight:
While the majority of respondents have a Process Improvement program in place, it was confirmed during the in-depth interviews that the work to acquire the data and put the data into an analytic is performed manually.
This can be a very resource-intensive process, depending on the capabilities of the ED’s staff and IT department’s availability to assist. And, it is further complicated by the interoperability challenges of Electronic Health Records and other hospital systems.
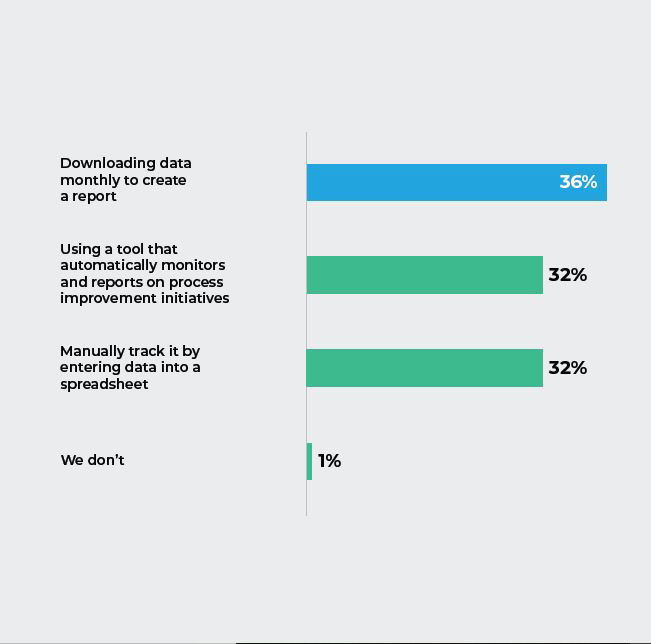
Q6. How do you monitor performance of any improvement initiatives implemented in your ED?
The Insight:
Respondents acknowledged that when doing the work manually, with limited data sets, performance analysis can only go so far. This not only results in lost time, but also in missed opportunities and insights into areas that could help improve performance.
Another recent study identified that a mere 5 percent of the responding organizations reported that they had succeeded at conducting what they considered “advanced analytics” which reveals that most HCOs still haven’t been able to convert their data into the asset they need it to be.
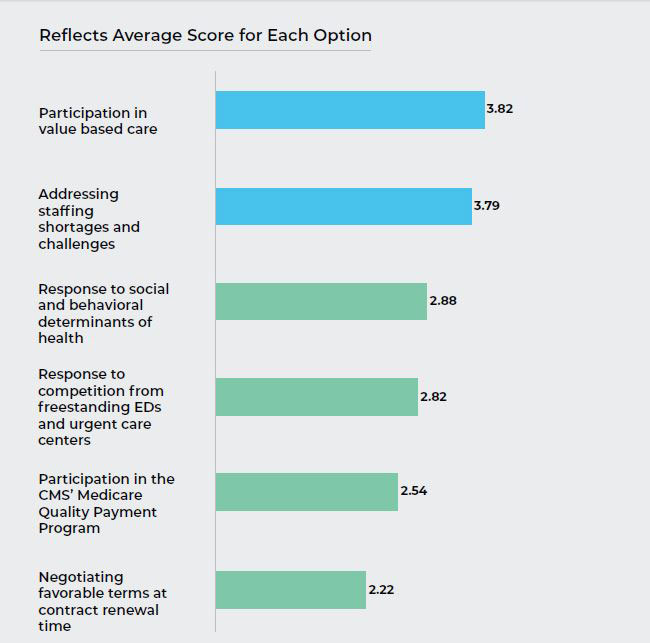
Q7. How would you rate the level of readiness in your ED for the following on a scale of 1 to 5, with 5 indicating total readiness?
The Insight:
The majority of respondents indicated an average or better level of readiness with regard to successfully responding to changes going on in the health care eco-system. While many respondents felt they were prepared, many were not prepared due to a lack of timely, relevant and actionable information. One area that many respondents felt less ready for was in responding to social and behavioral determinants of health where the number of patients arriving at the ED is on the rise.
While many acknowledged the importance of social and behavioral determinants on health outcomes, many lacked access to the necessary psych resources and felt that social determinants were largely out of their control. Utilizing advanced analytics there are opportunities for the ED to better make the business case for efficiently deploying needed resources.
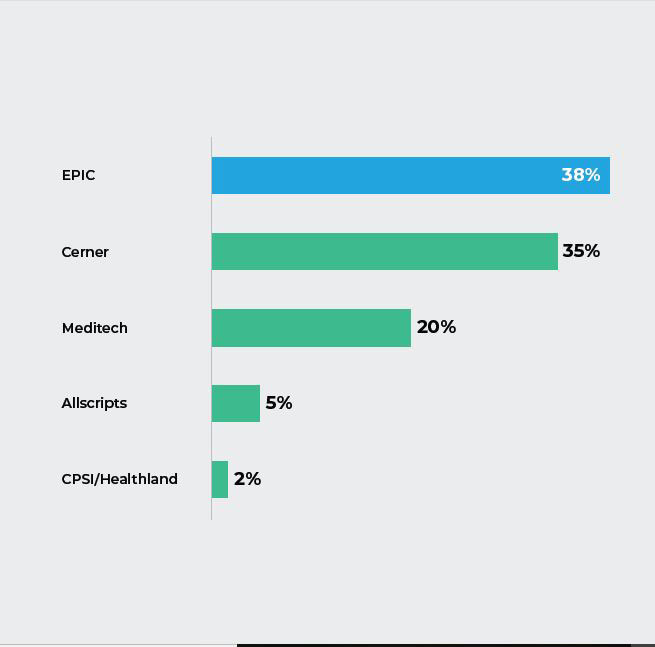
Q8. What EHR does your hospital use?
The Insight:
The majority of respondents stated they use Epic software for their EHR, with Cerner as a very close second. According to a recent American Journal of Emergency Medicine study, physicians spend nearly 44% of their time entering data into an EHR and see an average of 2.5 patients an hour.
Many health care organizations have recently updated their EHR systems in order to comply with the ACA and gain their incentives. While EHR vendors may have promised to solve all their interoperability, productivity, and analytics challenges, studies show that EHRs still lack sophisticated analytics functionality, leading to dissatisfaction and contributing to a growing desire to switch vendors.
Recent research indicates the number of health care organizations planning to switch HER systems or those in the process of switching has been growing in the past few years. A 2018 report by Black Book Market Research found that 22 percent of hospital IT managers reported that they will evaluate alternative EHR vendors in 2019. Another report indicated that more than
40 percent of the 127 health care organizations surveyed were either “dissatisfied with or indifferent” about their current EHR systems.
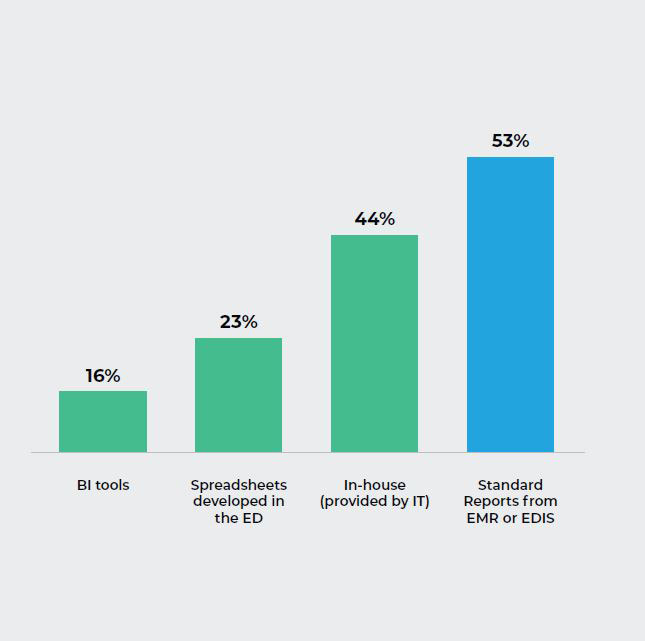
Q9. What service or application do you use for your ED’s key performance analytics?
The Insight:
Most respondents stated they use the standard reports that come from their EHR or EDIS systems for their performance metrics, with in-house IT reports as a very close second.
Performance measurement is a critical step in the feedback mechanism, helping a department understand how it is performing. While Hospitals have always been data-driven organizations, the availability of more data and new business imperatives, are becoming increasingly important when providing feedback to multiple stakeholders.
Q.10 How many FTE hours a month, would you estimate, are required to get your ED’s key metric performance analytic reports?
Comments:
- A lot of time. It changes depending on the needs of the department.
- It is outsourced
- Done by TeamHealth Data team. Measured per unit.
- Measured per unit. 2.66 hours per patient
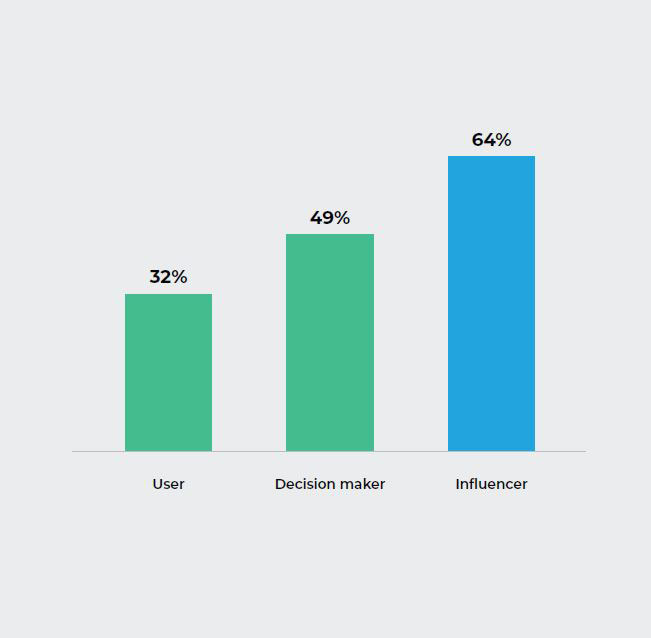
Q11. How are you involved in the decision to process relative analytics and performance reporting tools?
The Insight:
When it comes to the analytics and performance reporting tools decision process, most respondents cited themselves influencers.
Surprisingly, only 49% identified themselves as direct decision makers. This could tie back to Q7 while many acknowledge and are aware of the hindrances and determinants on health outcomes, they lack the access to the necessary resources and/or feel it is out of their control.
About d2i
d2i was founded in 2010 by Scott Richards and Jonathan Rothman, who each have more than 20 years of experience in EM data management and analytics. The company provides an ED analytic application that aggregates, harmonizes, and enriches data from various sources, and provides actionable insights that lead to ED performance optimization.
d2i provides vital services to many of the largest EDs in the U.S. with a cloud-based application that spans the clinical, quality, financial and operational domains.
d2i’s analytical application embeds best practices determined by details from more than 17 million ED visits. It requires little up-front cost and no new infrastructure and can be implemented in a matter of weeks.
In addition to its application, d2i offers analytic services, sharing its extensive industry expertise and organic knowledge to ensure that client partners continue to stay ahead of the curve by rapidly identifying and implementing opportunities for improvement.
Our Point of View:
To support value-based purchasing, performance improvement initiatives require that data be aggregated, harmonized, and analyzed from many perspectives – operational efficiency, cost, clinical practice variation, quality, and patient satisfaction. However, the effective implementation of rapid and continuous operational performance improvement has been elusive due in large part to the complexity of curating disparate data in order to make it fit for purpose. This data curation is necessary in order to understand the cause, effect, and impact various metrics have across domains. The ability to understand the impact of particular measures is key. Dr. Edwards Deming, the leading thinker on quality management, famously said, “Measurement without the opportunity to improve is harassment.”
Analytics itself does not inherently improve anything. It helps to identify opportunities for improvement. While analytics will be the key technology that will drive performance improvement initiatives, attack the 1B+ in waste, and improve population health, analytics in healthcare has overpromised and underdelivered. The antidote – Purpose-built performance analytics that is an organic product of the domain built for performance and process optimization.
The d2i solution is organically developed and improved through the collective wisdom and best practices of a community dedicated to similar goals. The d2i solution is the product of over 20 years of experience, working with and for ED stakeholders to give them a tool that works for them, not one that requires work by them. New analytics are created continuously as new questions, learnings and evidence based best practices emerge. To enable this approach d2i bridges the gap between data science and business domain expertise and provides the following services.
- Data acquisition services and solution accelerators for most source systems.
- Data harmonization services for normalizing, cleaning and enriching data.
- Curated and purpose-built data repository that supports the five levels of why without the need for data jockeying. The repository provides enough visits across sites to support statistically meaningful pattern recognition and benchmarking.
- On-going data quality services to rapidly identify data gaps and anomalies to ensure historical accuracy. This involves cross-referencing data across data sources (for example EHR and billing) to continually check for discrepancies. Confidence in data integrity is a must if it is to be used to enable performance improvement conversations.
- On-going support to the user community to ensure trends are understood, opportunities for improvement are reviewed and existing or organically developed new analytics are leveraged to identify and promote high impact actions.
- Highly adaptive process and HIPAA compliant cloud-based architecture allowing for the rapid inclusion of new algorithms and analytics.
- Local customization to allow for differences in site priorities and processes.
d2i’s success in Emergency Medicine has led it to provide the following product and services:
- Revenue Cycle Management Performance Analytics
- Hospital Medicine Performance Analytics
- MACRA MIPs Performance Analytics
- DAaaS (Data Acquisition as a Service)
- DaaS (Data as a Service)
For more information, contact us here www.d2ihc.com/contact